SLAP Tears

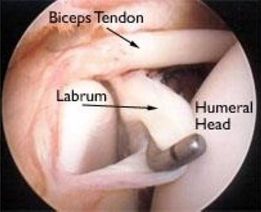
The shoulder is a complex are which consists of 5 joints, the main one being the glenohumeral joint (ball & socket) & is made up of 3 bones: the humerus, the shoulder blade, & the collarbone . The head of the arm bone articulates with the glenoid cavity (socket), around which is a strong, fibrous tissue called the labrum, which helps to cushion & deepen the socket, thus stabilising the shoulder joint. Ligaments & one of the biceps tendons also attach to the labrum, providing shoulder stability alongside the rotator cuff muscles.
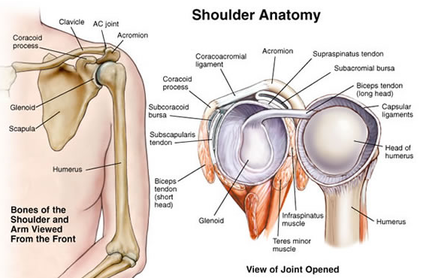
There are various types of labral tears, but a SLAP tear (Superior Labral Anterior to Posterior ) is where the labrum tears around the top,where the biceps tendon attaches, usually over a period of time.
RISK FACTORS:-
• repetitive overhead sports eg.baseball, swimming & weightlifting - the labrum gradually wears down because of overuse
• Ageing – more common in people over 40 due to wear & tear & the labrum being less firmly attached to the glenoid cavity
Research has shown that:-
• sports injury is the leading cause of SLAP tears
• 50% of SLAP lesions were 40 years old+ with signs instability after previous acute trauma, repetitive injury, fall on an outstretched arm, or an injury from heavy lifting. Most of these are type II SLAP.
• Type II SLAP lesions in patients under 40 are usually linked to bankart_lesion

CAUSES:-
• OVERUSE – repetitive overhead movements eg.occupational, weightlifters, swimmers, throwing athletes
• Hyperextension of the arm
• INJURY - eg.
- falling onto an outstretched arm
- shoulder dislocation
- car accident
- forceful pulling on the arm eg. catching a heavy item rapid/forced movement of the arm overhead
• WEAR & TEAR - especially aged 40 or older
• Bursitis and rotator cuff tears are often connected to SLAP tears
TYPES OF SLAP TEARS:-
• TYPE I - fraying of the top rim of the labrum, which is still attached to the glenoid/biceps tendon
- due to the ageing process (common in middle-aged/ older patients
- could be treated without surgery
• TYPE II - most common type of SLAP tear
- the labrum & biceps tendon detach from the top of the glenoid
- can be further identified as anterior,posterior or a combination.
- usually involves arthroscopic surgery
• TYPE III - a bucket-handle tear ie. the torn labrum can drop into the shoulder joint
- the biceps tendon remains intact
- usually requires arthroscopic surgery
• TYPE IV - a bucket-handle tear to the top of the labrum
- extends into the biceps tendon
- least common type of SLAP tear
• TYPE V - a Bankart lesion (due to dislocation) that extends superiorly to include a Type II SLAP
• TYPE VI - an unstable labral flap tear with biceps tendon separation.
• TYPE VII - a superior labrum and biceps tendon separation that extends anteriorly
SYMPTOMS:-
• Locking/ popping/ grinding/clicking sensation
• feeling that the shoulder is going to give way
• deep, aching shoulder pain when moving /lifting overhead
• pain is usually intermittent and difficult to pinpoint exact location
• pain may be felt around the front of the shoulder if the biceps tendon is affected
• pain when holding the shoulder in specific positions eg stretching the arm behind the head
• Reduced shoulder strength
• Reduced range of motion/ difficulty reaching and throwing
• Reduced throwing velocity
• “dead arm” feeling after throwing
• Reduced sports performance and power
• Inability to lie on the shoulder
Decreased functioning of the scapula often affects stabilising muscles such as the serratus anterior/rhomboids/ levator scapulae/ trapezius/rotator cuff.
TREATMENT
Treatment will vary according to the type of SLAP tear.
Nonsurgical Treatment
• Rest from any activities which aggravate the injury
• anti-inflammatories eg.ibuprofen to reduce pain and swelling
• intra-articular corticosteroid injections
• physical therapy 3-6 months to restore movement and strengthen the shoulder – exercises will be recommended to stretch the capsule of connective tissue surrounding the joint and to strengthen the supportive muscles, such as the rotator cuff,deltoid and even the muscles of the torso that help stabilise the shoulder
Surgical Treatment
-may be suggested if pain doesn’t improve with nonsurgical treatment
Arthroscopy will be done to determine the best course of action,dependant on the type of tear, age,activity level etc, which may involve any of the following:-
• removing the torn part of the labrum
• reattaching the torn labrum with stitches
• cutting the biceps tendon attachment Wearing a post surgical sling for approximately a month will protect the shoulder.
RECOVERY
Recovery time varies and full recovery may take several months, potentially 2 months for the labrum to heal and 2 more months to return to previous strength. Aside from some gentle exercises to improve flexibility, actual muscle strengthening exercises usually aren’t started until around 4-6 weeks post surgery. Return to sports activity will depend on the type of tear, pain levels etc,. but throwing athletes can usually start to return 3 to 4 months after surgery, even though full healing usually takes around 6 months.

EXERCISES
Exercises to stretch the posterior capsule:-
• sleeper stretch
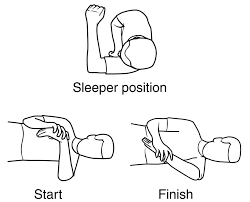
• cross body adduction stretch

TORN LABRUM EXERCISES WITHOUT SURGERY:-
If surgery isn't required, focus on exercises that increase flexibility,strengthen the rotator cuff muscles and the shoulder blade stabilizing muscles.
STRETCHING THE SHOULDER:-
-Wall stretches
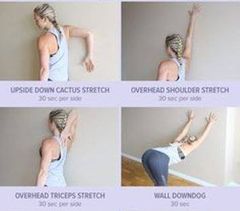

-Anterior shoulder stretch

-Hand up your back stretch
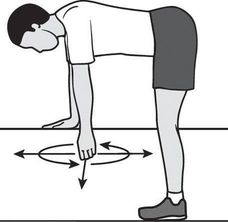
-Pendulum exercises
EXERCISES TO STRENGTHEN THE SHOULDER:-
-Shoulder blade retractions
-Isometric shoulder exercises
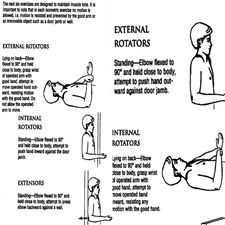
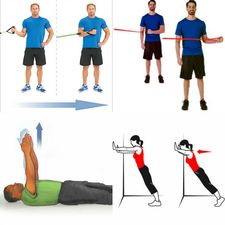
-Internal and external rotation exercises using a band
-Wall push-ups
-Arm reach
TORN LABRUM EXERCISES POST SURGERY:-
• 0-2 weeks after surgery you can do pendulum exercises
• Shrug shoulders in an upward movement.
• Pinch shoulder blades backward and together
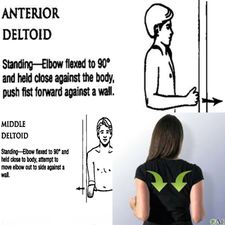
• Isometric internal and external rotation: While facing wall, keep elbow against your side and hold your forearm at 90 degrees. Place the palm against the wall with the thumb facing up (for internal rotation) or the back of the hand against the wall with the thumb facing up (for external rotation). Pull or push against the wall.

• Squeeze a rubber ball and hold for five seconds
• Supine passive arm elevation: Lying on your back, hold the injured arm at the wrist with the opposite hand, lift the injured arm upward, then slowly lower it back down.
• Hand up back stretch