Meniscal Tears

ANATOMY OF THE KNEE & MENISCUS
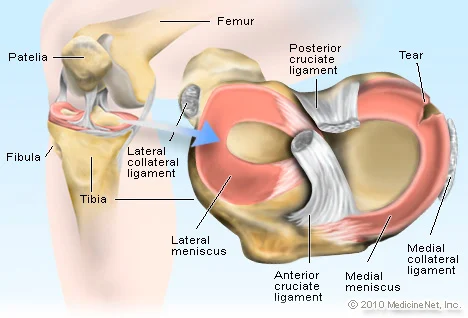
The femur, tibia and patella bones are held together by the ligaments of the knee, forming a hinge joint, and although incomplete in places, the articular capsule of the knee is strengthened by ligaments and tendons.
The knee has two menisci, or fibrous cartilage that sit between the bones,which have the following functions:-
• cushion the joint between the femur and tibia
• absorb any impact on the knee
• stabilise the knee and accommodate smooth movement
• help regulate the flow of synovial fluid, protecting the knee from wear and tear
• help balance out the weight distribution of the knees
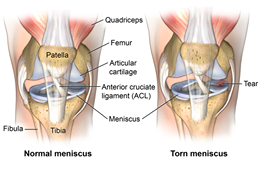
The two menisci, the medial and lateral, change position slightly when the knee moves, and if too much weight is placed on a partially flexed knee, the meniscus may get caught between the tibia and femur bones, causing a tear. Given that the menisci only have a blood supply at their outer edges, if they tear, healing can take some time.
Meniscus tears are a common injury in sports due to the knee having to support a lot of weight during jumping and running or supporting heavy weights at the gym. Treatment and recovery will be influenced by severity and location of the tear, and how old and active the person is.
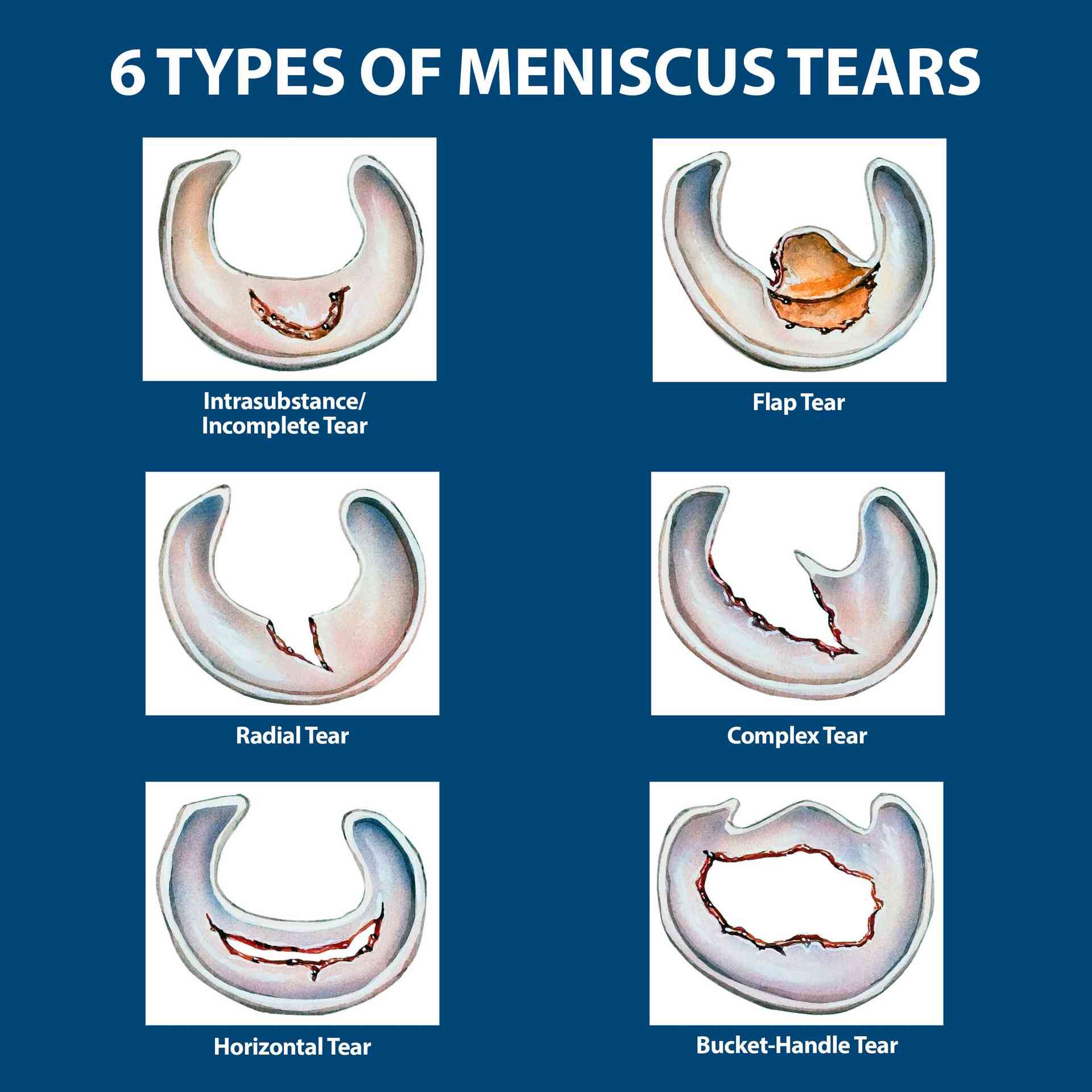
TYPES OF MENISCAL TEAR
The medical meniscus, on the inside of the knee forms a ‘c’ shape, while the lateral meniscus on the outer knee, forms a ‘u’ shape, and pain will affect the inner or outer knee depending on which meniscus is torn.
SYMPTOMS, COMPLICATIONS AND TREATMENT SYMPTOMS
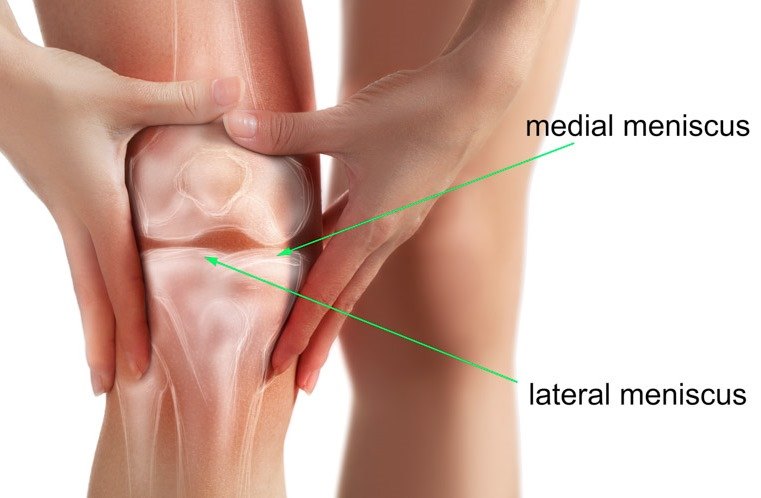
• severe pain, particularly when trying to straighten the leg or when touched (this may be medial or lateral depending on which meniscus has torn)
• an initial popping sound around your knee joint at time of injury
• mild to severe swelling of the knee – due to accumulation of fluid
• reduced range of motion and difficulty walking
• periodic collapsing of the knee while walking
• a feeling that the knee will collapse when walking
• clicking at approximately 30 degrees before full extension
• periodic sticking of the knee in a bent position – due to cartilage folding and blocking the normal movement
• pain and swelling may temporarily subside upon jiggling the knee if the cartilage has folded, as this may return cartilage to its normal position
• if the knee locks in a straightened position and bending the knee is not possible, seek medical attention
COMPLICATIONS IF UNTREATED
• can cause premature wear and tear and arthritis • irregular cartilage edges or folded cartilage may cause locking of the knee • part of the meniscus may come loose and become trapped in the joint • tears can increase in size • following total or partial menisectomy – the meniscus may be removed due to lack of blood supply to this area affecting healing, but this can impact on knee stability

IMMEDIATE NON SURGICAL TREATMENT
Treatment will vary according to the type and location of meniscal tear, the persons age and activity level and their symptoms, eg. a small tear on the outer edge can heal with minimal treatment due to there being a blood supply in this area. A tear on the inner edge of the meniscus does not have this blood supply, so will usually need surgical treatment.
• RICE (Rest, Ice , Compress, & Elevate) - to reduce swelling and control pain
• wearing an elastic compression bandage, brace or using crutches to limit weight bearing, swelling and movement may be advised
• Anti-inflammatories
• avoid any activity/weightbearing that makes the pain worse
• electrical stimulation —may be used to strengthen the meniscus and surrounding tissues
• Corticosteroid injections - to relieve pain or inflammation temporarily, but may still require meniscus surgery
• PRP (platelet rich plasma) injections at the site of the tear,releases growth factors to stimulate healing
• massage to reduce swelling and stiffness
• physiotherapy to restore functionality and strength, and improve stability
Physiotherapy may be part of a conservative treatment plan, or be used in both preparation for and recovery from surgery, helping to strengthen and stretch the muscles around the knee to avoid overcompensatory imbalances.
ARTHROSCOPIC SURGICAL TREATMENT
Doctors may wait for about six weeks to see if swelling and pain improve before treating surgically, which may involve any of the following:-
• medial or lateral menisectomy (removal of meniscus)
• partial or total menisectomy
• meniscus repair - if the tear is in the outer red zone,which has a good blood supply (about 6 weeks recovery)
Surgery is much more likely if the knee keeps locking.
REHABILITATION,EXERCISES & MASSAGE REHABILITATION

· may take from 3 weeks to 3 months, depending on the type of tear
· pivoting, twisting and squatting movements should be avoided
· exercises to improve range of motion start within a few days of surgery
· Exercises to maintain quadricep muscle strength for knee stability (initially straight-leg raises or mini-squats which only bend the knee to about 15 degrees)
· crutches to help with walking until healed
PREVENTION
· perform exercises regularly that strengthen the leg muscles to help stabilize the knee joint
· use protective sports equipment or a brace to support the knee during activities that may increase your risk of injury eg.deadlifts
· use correct technique when doing exercises that may put the knee under pressure
· warm up and stretch before exercising
· wear shoes designed for the activity
EXERCISES FOR RECOVERY PERIOD
· FLEXION/EXTENSION— bending and straightening the knee as far as pain and range of motion allows, initially only 15 degrees of flexion
· STRAIGHT LEG RAISES — lying on your back with uninjured knee bent upwards while keeping the injured leg straight and on the ground, slowly lift the leg about six inches off the floor,tightening the quad muscles
· HEEL SLIDES — lying on your back slide the heel of the injured leg along the ground, moving as near as possible towards the buttocks (again only as pain allows and the degree of flexion will be minimal to start with)
· CALF RAISES — stand with feet shoulder width apart, lift heel up as high as possible off the floor and slowly back down (only as pain allows and the degree of flexion will be minimal to start with)
· HIP ABDUCTION — stand on uninjured leg and raise the injured leg out to the side as far away from the body as possible
PRECAUTIONS
· take time to recover and slowly gain back strength
· start with basic stretches before progressing to more advanced exercises with weights and deeper squats
· stop exercises if causing pain
MASSAGE
A variety of techniques can be used with sufficient pressure to reach the underlying structures of the knee through the superficial tissue. Myofascial massage may be particularly beneficial.
· increases blood flow
· reduces inflammation
· reduces pain
· reduces muscle spasm
· promote normal tissue repair
· breaks down scar adhesions – through deep frictions across the tissue as deeply as possible, this may be painful so only as much as pain levels allow
· restores normal range of motion
· stabilises the knee joint by helping to strengthen the muscles around the knee