- 07736 104738
- sam@medicalmassagelady.com
- Mon - Sat, 8:00 - 18:30

Frozen shoulder is where the shoulder joint gradually becomes painful and stiff for no apparent reason, getting worse and then finally disappearing in anything from 1 to 3 years. Usually only one shoulder is affected and loss of motion may be partial or complete, but if untreated will almost certainly get worse.
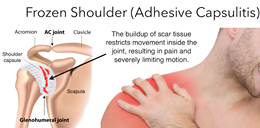
The shoulder is a ball-and-socket joint and the surrounding tissue is called the shoulder capsule. The ball and socket joint allows forward, backward, rotational and extension movements, so synovial fluid within the capsule protects the joint and helps maintain fluid movement. The capsule is also surrounded by ligaments, tendons, fluid-filled sacs (bursae) and the rotator cuff muscles, which while maintaining flexibility, also makes the joint vulnerable to trauma. When this protective capsule contracts and stiffens, the shoulder becomes frozen, and scar tissue forms between the joint capsule and the head of the humerus, due to a lack of synovial fluid to lubricate the joint.
While not fully understood, this contraction of the capsule is most likely due to the inflammatory process and long term immobility from injury, surgery, or illness. Overuse injuries such as bursitis or tendinitis of the rotator cuff are likely to be a common factor. Efforts to avoid painful movement then lead to further contraction of the capsule.
While a frozen shoulder can get better by itself, this can take up to 3 years, so treatment is advised to improve range of motion and ease pain. It is very uncommon to have frozen shoulder more than once in the same shoulder.
ALTERNATIVE DIAGNOSES:-
• ROTATOR CUFF INJURY - only painful with active movement, not with passive movements
Both active and passive movements are painful with a frozen shoulder
• osteoarthritis of the shoulder
• tendonitis of the biceps tendon
• inflammation of the bursa under the collarbone around the shoulder (subacromial bursitis)
• rheumatoid arthritis of the shoulder

RISK FACTORS:-
• affects about 3% of adults at some stage in their lives
• more common in women than men, between the ages of 40 and 60
• most commonly affects the non-dominant shoulder, with 1 in 5 cases also developing in the other shoulder at some stage
• following a shoulder injury – 10%of people with rotator cuff disorders develop frozen shoulder
• lack of exercise after tendonitis or injury or wearing a sling without intermittent stretching
• recovering from a medical condition that prevents movement of the arm eg a stroke, or mastectomy
• certain medical conditions eg. heart disease, thyroid disease, Parkinsons disease
• 10% to 20% of people with diabetes get frozen shoulder
CAUSES:-
No definitive cause has been identified, but the following have been linked:-
• STROKE - research shows that 72% of stroke victims experience frozen shoulder due to immobility
• BROKEN ARM – treatment and recovery can take months and trauma that is enough to break bones can cause the protective tissues around your shoulder joint to thicken
• ROTATOR CUFF INJURY - help to keep the arms and shoulder connected, and stabilise the shoulder but it is prone to injuries due to being exposed to high impacts
• SURGERY RECOVERY – due to immobility or scar tissue
• DIABETES - diabetes can affect the skeleton in various ways and the shoulder joints are often targeted
• HEART DISEASE - due to disruption of blood flow and nutrients around the body
• UNDERACTIVE THYROID - releases hormones that affect the metabolism and imbalance of these hormones can result in various symptoms including weight gain, stiffness, weakness and fatigue
• OVERACTIVE THYROID - releases too many hormones causing anxiety, rapid heartbeat and affecting joints and muscles
• PARKINSON’S DISEASE - neurodegenerative disorder causing loss of mobility, tremors and difficulty balancing
• TUBERCULOSIS - mostly affects the lungs but can infect other parts of the body causing fatigue.
DR AUSTIN OOLO’S PERFECT STORM THEORY
This theory suggests that there is a “perfect storm” of 3 issues that occur simultaneously causing frozen shoulder.
· LOWER NECK DISC PATHOLOGY OR NERVE COMPRESSION – xrays show that frozen shoulder almost always occurs alongside lower neck disc conditions, degenerative changes at C5-6 being very common, or muscle conditions which compress the nerves in the lower neck that supply the shoulder & arm with motor & sensory information
· HORMONAL IMBALANCE - frozen shoulder always occurs alongside hormonal imbalances eg. menopause, diabetes, thyroid, adrenal stress, testosterone imbalance, or chronic stress which impairs adrenal function & increases cortisol levels. Hormonal imbalances eg.menopause, can cause increased scar tissue formation, meaning that even a minor injury of the shoulder muscle may not heal so well due to an uncontrolled immune healing response
· SHOULDER STRAIN INJURY - those with frozen shoulder usually wake up one day with a stiff & painful shoulder, which can often be related back to a strained muscle a few days before, maybe lifting something awkwardly or sleeping in an odd position. This initiates the inflammatory response
The theory is that nerves in the lower neck are compressed by an issue with a cervical disc or the neck muscles, causing motor signal transmission problems to the muscles in the shoulder. This causes weakness in the shoulder muscles. If severe, symptoms such as neck or shoulder pain, headaches or numbness in the hands will be present but otherwise the compressed nerves go unnoticed.
If a muscle injury is involved, the inflammatory response kicks in to promote healing, overseen by the immune system which is linked to the hormonal system. Inflammation peaks at 3-4 days after injury, explaining why people suddenly wake up feeling stiff.
Normally, contraction of the shoulder muscles against a resistive load may then stress the muscle causing a tear in the muscle, tendon or shoulder capsule. Swelling generally protects the area from further injury & promotes the hormone secretion to allow healing. Stronger tissue re-bonds the torn tissue forming scars & adhesions.
With frozen shoulder, the inflammatory response is much stronger due to a hormonal imbalance, which also causes an imbalance in the immune system. The healing response will then be over-exaggerated, forming excessive scar tissue across the shoulder capsule.

SYMPTOMS
Symptoms will only be experienced in the shoulder, usually only one is affected. Everyday activities eg. driving, dressing, or sleeping can become difficult. If untreated, symptoms may last 2-3 years before going. The main symptoms are:-
• dull, aching pain in one shoulder, possibly around the top of the arm
• pain may get worse at night causing sleeping problems
• stiffness and sometimes complete loss of mobility
3 STAGES OF FROZEN SHOULDER:-
• FREEZING STAGE – usually lasts 2-9 months. Pain is noted first and then limited movement. Symptoms gradually worsen, particularly with movement or when lying on that shoulder at night.
• FROZEN STAGE – usually lasts 4-12 months. Pain will gradually ease whereas the stiffness tends to worsen, affecting all shoulder movement, particularly external rotation of the arm. The shoulder muscles may start to atrophy due to lack of use
• THAWING STAGE – recovery stage usually lasts 1-3 years. Pain and stiffness gradually disappear and normal range of motion is restored.
TREATMENT
Certain movements such as reaching across the chest to touch the opposite shoulder or down your back to touch the opposite shoulder blade are characteristic of a frozen shoulder. There is a chance your shoulder will get back to normal without treatment but this can take a couple of years, so most people like to find some kind of treatment option to help ease symptoms.
• ANTI INFLAMMATORY PAINKILLERS - eg ibuprofen, diclofenac, naproxen. These should really only be taken in the initial part of the freezing stage to reduce inflammation, and given the theory of hormonal influence, it is important to be aware that these drugs can affect the kidneys. If there is any kind of adrenal gland issue or diabetes, therefore, it would be better not to take these.
• SHOULDER EXERCISES – will help to reduce any further stiffness and maintain as much movement as possible
• PHYSIOTHERAPY – may advise on exercises and other pain-relieving techniques such as warm or cold packs and TENS machines
• STEROID INJECTION – can relieve symptoms for several weeks and reduce inflammation. However, these injections can damage the tendons inside the shoulder, introduce infection or cause bleeding.
Also given the perfect storm theory which includes chronic stress in the hormonal issues, due to cortisol release, this may not be the best option
• HORMONAL TREATMENT – if you are aware of/suspect any hormonal imbalance or suffer from medical issues affecting the hormones, eg. diabetes, it may be wise to get some blood tests done to check the levels and ensure that any treatment for that issue is sufficient
• JOINT DISTENSION - injection of sterile water into the shoulder capsule to stretch it, in order to improve movement
• SURGERY – may be considered if other treatments do not help but can damage the shoulder elsewhere.
This may involve:-
- MANIPULATION - the shoulder is mobilised under anaesthetic to release scar tissue but this carries a risk of damaging other parts of the shoulder
- ARTHROSCOPIC CAPSULAR RELEASE - the tight capsule of the joint is released with a probe
• DO NOT IMMOBILISE THE SHOULDER – using a sling in an attempt to support the shoulder will actually make recovery harder and encourage further stiffness
• MASSAGE THERAPY – to strengthen and stretch the tissues, encouraging mobility
EXERCISES
Warming up the shoulder by taking a warm shower or bath for 10 - 15 minutes before performing exercises is recommended, or alternatively you can use a warm pack.
If the frozen shoulder is severe, the active range of motion (ie. movement that can be performed individually, without assistance) is less than passive range of motion. Consequently, many exercises use the healthy arm, or a pole for assistance. When performing exercises, stretch to the point of tension but not pain.
Any activities requiring overhead reaching/lifting, or that increase pain should be avoided. At least 90% of people improve with these exercises but full recovery takes months to years.
• PENDULUM STRETCH

– starting exercise. Stand and lean over slightly, shoulders relaxed, allowing the affected arm to hang down. Swing the arm in a small circle — about a foot in diameter, 10 times in each direction. As your symptoms improve, increase the diameter of your swing, and then eventually you can hold a 3-5lb weight
• SUPINE FLEXION

– lay down flat with arms at the side of the body, then using the healthy arm for assistance, lift the injured arm vertically in the air and backward to the floor with the help of the healthy arm. Keep reaching until a stretch is felt, eventually lifting the injured arm overhead
• STANDING EXTENSION

– stand, holding a pole horizontally behind the body, arms shoulder width apart with knuckles facing toward the ground. Lift the arms in an upward movement until a stretch is felt. Repeat 10 times, holding for 1 - 5 seconds
• CROSSBODY STRETCH

- sit or stand with both arms relaxed at the sides. Bring the affected arm across the chest, supported by the healthy arm at the elbow. Hold for 15 - 20 seconds.
• DOORWAY PASSIVE EXTERNAL ROTATION
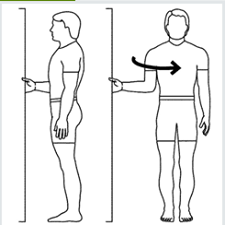
- Stand, facing one side of the doorframe. Bend the affected arm to a 90-degree angle and grab the edge of the doorframe with the hand of the affected arm. Rotate the body so the backside is now in the doorway. Hold for 30 seconds then repeat.
• TOWEL STRETCH

- hold a rolled towel with both hands behind your back in a horizontal position. Use the good arm to pull the affected arm upward to stretch.
• ARMPIT STRETCH

- lift the affected arm onto a shelf about breast-high, and slowly bend your knees, opening up the armpit. Deepen your knee bend slightly, gently stretching the armpit, and then straighten. With each knee bend, stretch a little further. Once the range of motion improves, you can move on to the following exercises to strengthen the rotator cuff.
• OUTWARD ROTATION

- hold a resistance band between your hands with your elbows at a 90-degree angle close to your sides , then rotate the lower part of the affected arm outward 2-3 inches and hold for 5 seconds. Alternatively you can attach one end of the band to a door handle on a closed door.
• INWARD ROTATION

- stand next to a closed door, and hook resistance band around the door handle. Hold the other end with the affected side, holding the elbow at a 90-degree angle. Pull the band toward your body 2-3 inches and hold for 5 seconds.
HOW DOES MASSAGE HELP A FROZEN SHOULDER?

Massage is often used by those with frozen shoulder at some point works by improving blood circulation and nutrient supply which assists with healing, relaxing and improving mobility of the stiff shoulder muscles and breaking down scar tissue. Various techniques can be used to treat frozen shoulder and regular massage is necessary to keep on top of the symptoms.
• SWEDISH MASSAGE - relaxing strokes and kneading can help alleviate the tension within the surface muscle tissues, but in my experience a frozen shoulder requires deeper work to really access the scar tissue and soft tissues around the shoulder capsule.
• DEEP /SPORTS MASSAGE - consistent pressure on the muscles can release the scar tissue causing the pain. However, this is best avoided if still in the inflammatory phase as it can cause more pain
• TRIGGER POINT THERAPY- the steady pressure being applied to specific points on the muscles can ease muscle spasms and pains.
• HEAT THERAPY - before or after the massage will help relax the affected muscles, further relieving the tension and pain.


