- 07736 104738
- sam@medicalmassagelady.com
- Mon - Sat, 8:00 - 18:30

When the bone segment distal to a joint sits at an outward angle, away from the body's midline, this is known as a valgus. When the angle is inward, toward the midline of the body, this is called varus.
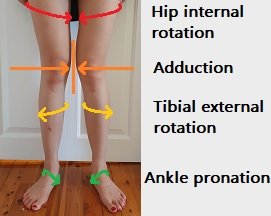
Knee valgus is characterised by the inward bending of the knees, when structural deformity or muscle/ligament weakness causes internal rotation of the hip and femur. Instead of facing forwards, the knees will point towards each other. The tibia (shinbone) may then compensate by externally rotating.
While generally seen in children, valgus deformities may continue into adulthood. 20% of children under the age of 3 having >0.4 inch space between their ankles, but this usually corrects itself. By 7 years old, this reduces to only 1%. In rare cases, usually where there is an underlying condition, knee valgus may continue into adolescence or develop in adulthood.
CAUSES
• structural deformity – of the knee, femur, tibia, rickets
• flat feet
• traumatic injury
• arthritis in the knee (rheumatoid and osteoarthritis)
• muscle imbalance due to poor posture
• genetics
• poor posture
THE EFFECT OF POOR POSTURE ON KNEE VALGUS
There are various muscles which stabilise and enable full range of motion in the knee.- the hip abductors, external rotators, quads, and hamstrings. Dealing with any muscle weakness is vital to ensure proper knee alignment which means that weight is evenly distributed through the hips, knees, and ankles.
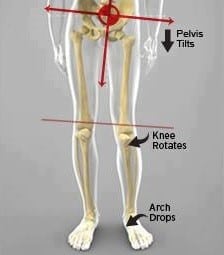
With knee valgus, there is external rotation due to hip weakness and internal rotation of the femur due to the hip abductors, and pelvic muscles.
• tight adductors – if these inner thigh/groin muscles are too tight, they will pull the thighs inwards and internally rotate the hip
• weak abductors – weakness in the gluteus minimus and medius, and the tensor fascia latae , mean that alongside tight adductors, there is a greater inward pull than outward, drawing the knees inwards
• flat feet – cause poor alignment of the knee through over pronation and generally present in those with valgus of the knees
• naturally wide hips – people with wider hips, generally women, seem to be more likely to develop knee valgus., as this promotes internal rotation
• anterior pelvic tilt – when the pelvis tilts downwards at the front, this can encourage internal rotation Identifying the cause of knee valgus is essential in finding an effective treatment, but when the issue can be with the ankles or the hips this may not be an easy task, however, if poor posture is recognised as the problem early on, then the valgus can be corrected.
SYMPTOMS
• knock-kneed appearance - when standing with legs together the ankles will have >2 inches between them
If left untreated, valgus may progress and cause:-
• altered gait
• limping
• reduced range of motion
• difficulty maintaining balance
• hip, knee, ankle and foot pain (although pain generally isn’t a symptom unless untreated)
• low back pain
• swelling or buckling of the knee – usually occurs with underlying condition
COMPLICATIONS
If untreated, knee valgus can increase the risk of meniscus tears, joint damage, and osteoarthritis
TREATMENT
Knee valgus caused by structural deformities can’t be fixed or prevented and treatment will focus on reducing symptoms, whereas posture related valgus can be corrected.
• medication – to treat underlying conditions or manage pain in more serious cases
• surgery – may involve a plate being inserted to correct the knee alignment or realignment of the femur to correct the angle
• arch supports and insoles - to counterbalance altered walking patterns and additional pressure on the knees, hips and ankles due to flat feet
• massage/exercises – in postural cases to strengthen weak hip external rotators and hip abductors, restore flexibility to the hips and lengthen tight adductors

PREVENTION
• knee valgus due to a structural deformity can’t be prevented, but if due to posture:-
• fix muscle imbalances through massage or exercise before they become a problem
• maintain a healthy weight - obesity increases pressure on the legs and knees
• avoid hyperextending the knees as this can damage the medial collateral ligament (MCL), which helps prevents inward buckling, and the anterior crucial ligament (ACL), which stabilises the knee in rotation
• maintain good sitting posture with knees bent at 90-degrees angle and feet flat on the floor. Do not sit with your knees together and ankles apart
• ensure good technique when working out, particularly with squats, lunges and other exercises that can place stress on the knee and have potential for inward buckling

MASSAGE FOR KNEE VALGUS
It may be useful to begin some regular sports massage sessions with a sports therapist to:-
• STRETCH TIGHT ADDUCTOR MUSCLES – tightness here can cause inward buckling of the knees but myofascial techniques can lengthen and release them. Foam rollers may be an option but massage will be more effective
• STRENGTHEN WEAK ABDUCTORS – weak glutes and tensor fascia latae allow tight adductors to pull the leg inwards, but sports massage can correct such muscle imbalances
• ASSESS FOR ANTERIOR PELVIC TILT – offer corrective exercises and manipulation to stabilise the pelvis and avoid internal rotation of the femurs
• INCORPORATE TRIGGER POINT THERAPY INTO MASSAGE – may help ease any pain, and restore symmetry to the soft tissues and joints
EXERCISES

STANDING ADDUCTOR STRETCH– standing with feet around 3ft apart, shift your weight to one side and allow your knee to bend, keeping the opposite knee straight to feel a stretch on the inside of your thigh. Hold for 20 seconds and repeat on each side
SIDE-LYING LEG RAISES- Lie on your side and lift the leg away from your body, keeping toes pointed, and then back down. Repeat x30 each leg.
SIDE PLANKS WITH LEG RAISE- side planks where the top leg is raised can be difficult when your abductors are weak, but this is a good exercise to progress on to
BANDED SQUATS– doing squats with a resistance band means that you have to push the knees against the band, which works the abductors and encourages proper technique
VARUS KNEE/GENU VARUM/BOW LEGS

Varus knee occurs when the tibia (shinbone), turns inwards and is misaligned with the femur (thighbone), causing the knee to face outwards instead of straight ahead. If the tibiofemoral alignment is not 180 degrees, symptoms can arise after many years.
CAUSES
- Vitamin D deficiency resulting in rickets
- Newborns- bones haven’t yet moved into their permanent position. Children generally outgrow varus knee and develop a healthy alignment of the knee
- osteoarthritis – can cause the leg to bend outwards due to cartilage degeneration in the knee. However varus knee also causes osteoarthritis due to tibiofemoral misalignment
- Paget’s disease
- Bone tumours and infections
- Achondroplasia
- brittle bone disease - injury
- Blount’s disease- growth disorder of the shinbone
SYMPTOMS
- Bowlegged appearance
- pain on the inner knee in adults
- children may be asymptomatic
- joint pain if untreated
- cartilage degeneration in the knee, if untreated, which may develop into osteoarthritis
TREATMENT
- vitamin D/calcium supplements for early stage rickets
- surgery – osteotomy reshapes and realigns the tibia bone
- physical therapy and weight training to strengthen the surrounding muscles


