Femoroacetabular Impingement

FAI was recognised as a cause of osteoarthritis in the hip by Dr. Reinhold Ganz, an orthopaedic surgeon in 2003, while developing an open surgical dislocation procedure, but femoroacetabular damage has been recorded for over 100 years.
ANATOMY
The hip is a ball-and-socket joint, which enables multidirectional movement and rotation, between the femur and pelvis. The acetabulum of the pelvic bone forms the socket and is lined with strong fibrocartilage called the labrum which stabilises the joint by providing a tight seal . The head of the femur creates the ball and is covered with articular cartilage to provide a smooth, low friction surface that promotes easy movement. The hip joint has a complex musculature and major nerve supply from the femoral and sciatic nerves.
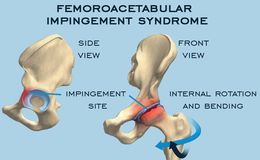
WHAT IS FAI? FAI occurs when there is abnormal movement between the hip bones due to development of bone spurs around the femoral head and/or the acetabulum, which can lead to labral tears and articular cartilage deterioration (osteoarthritis). It is one of the most common causes for hip pain in young/middle aged adults.
TYPES OF FAI
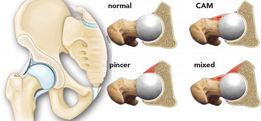
1)CAM IMPINGEMENT
- the head of the femur (ball) is not round so doesn't rotate smoothly within the acetabulum
- a bone spur on the upper edge of the femoral head (cam deformity) grinds the cartilage
- linked to development of osteoarthritis
2)PINCER IMPINGEMENT
- bone spur extends past the normal rim of the acetabulum (pincer deformity)
- can cause the labrum to be pinched under the prominent rim of the acetabulum
3)COMBINED IMPINGEMENT
- both the pincer and cam types are present
- occurs in approximately 70% of cases
Cam impingement occurs more often in males, while pincer impingement is more common in females due to anatomical differences in the pelvis.
CAUSES
- abnormal development of the hip bones during the childhood, leading to cam or pincer deformity, which causes joint damage
- many people are asymptomatic but when symptoms occur there is certainly cartilage damage to the cartilage
- high incidence in young, white athletes where the hip is subjected to forced, loaded flexion and internal rotation eg. in hockey, football, equestrian sports
- possible genetic link - increased incidence in siblings
- repetitive or prolonged squatting, twisting of the hip, getting in and out of cars, and sitting for prolonged periods
DIFFERENTIAL DIAGNOSIS
FAI can often be mistaken for the following:-
- piriformis syndrome
- labral tear without FAI
- adductor muscle strain
-sciatica
- athletic pubalgia (sports hernia/Gilmores groin)
- gluteus medius/minimus or illiopsoas tendinopathy
- stress fracture
- femoral head osteonecrosis
- other impingements
- anterior inferior iliac spine, ischiofemoral and iliopsoas
- loose body in the joint (intra-articular body)
SYMPTOMS
- pain in the groin area or outside of the hip (sometimes in upper buttock, lower back or below the buttock and posterior upper leg)
- stabbing pain when twisting or squatting
- stiffness, decreased movement
- limping
- symptoms may be sudden or gradual onset
- symptoms worsen with prolonged sitting
- if you get pain when bringing your knee up towards your chest and rotating it inward towards your opposite shoulder, impingement is most likely
TREATMENT
- avoid activities that cause symptoms
- anti-inflammatories to help reduce pain & inflammation
- ice packs may help ease inflammation
- seek medical attention if symptoms persist, to avoid further damage
- physiotherapy/sports therapy
- exercises/massage may improve the range of motion in your hip, strengthen the muscles that support the joint and improve posture, thus relieving some stress on the injured labrum or cartilage
- cortisone /hyaluronic acid injections
SURGERY
- recommended when symptoms persist despite conventional treatments
- corrects bony abnormalities which cause the impingement
- corrects soft tissue lesions eg labral tears - corrects the fit of the femoral head and acetabulum, reducing contact to improve range of movement
- usually done arthroscopically due to reduced complications and positive outcomes
- involves shaving of the femoral head, trimming of the acetabulum and labral repair
OUTCOMES
- while surgery can reduce symptoms and prevent further damage to the hip joint, severe damage due to delayed treatment may not be completely fixed by surgery - most athletes return to their previous level of activity
HOW MASSAGE CAN HELP
While massage can not be used as a stand alone treatment in FAI, it does have some benefits when combined with other treatment options:-
⦁ friction therapy helps reduce adhesions that form with repetitive injuries, causing pain and stiffness. Scar tissue thickens tendons, increasing risk of impingement
⦁ help restore range of motion through gentle stretching and myofascial release techniques, which can loosen connective tissue around the impingement,
⦁ helps to correct dysfunctional muscle patterns that may occur as a result of the pain and altered movement patterns
⦁ beneficial in controlling chronic pain , thus promoting recovery
⦁ helps to strengthen muscle tissue, helping to reduce further injury
EXERCISES
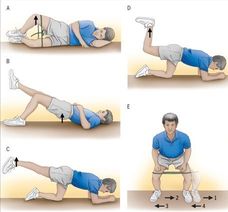
A) CLAMS - lying on side with knees bent, externally rotate the top leg upward, keeping feet together
B)SINGLE LEG BRIDGE - lying on your back with one knee bent and other leg straight, lift buttocks off the floor using the leg that is bent
C/D) HIP EXTENSION EXERCISES - on all fours, extend one leg upward, keeping knee slightly bent if initially too difficult to keep leg straight
E)SIDESTEP - take small steps sideways while keeping the toes pointed forwards and maintaining a slight squat Once pain subsides and these exercises are easy, you can use a resistance band to work harder.