
Massage for Cerebral Palsy – the demand for more therapists

In this article Sam Mishra aim offers a greater understanding of cerebral palsy and the gait patterns that can be helped through massage, alongside the other disciplines that will be in place.
Cerebral palsy (CP) is an umbrella term covering various brain injuries occurring during foetal development, birth and early infancy, which are categorised according to the area of brain damage. It is not a progressive disease but will affect development of motor skills and sensory and cognitive responses.
Approximately 1800 babies and infants are diagnosed annually, equating to 2-2.5 in every 1000 children in the UK. This means that there are approximately 30,000 children with cerebral palsy in the UK, and even more adults. While there will be input from physiotherapy, occupational therapy, podiatry and other professionals, I know only too well, having been the mother of a child with cerebral palsy, how limited these resources are.
Many parents therefore are turning to private therapies to help their children reach their full potential. With the right training, massage therapists, particularly those who are sports trained, are in the perfect position to provide therapy for this type of client, yet it doesn’t seem to be a common choice for therapists to specialise in.
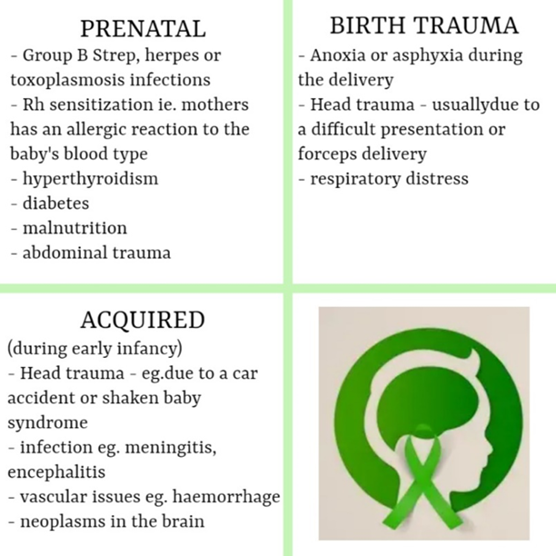
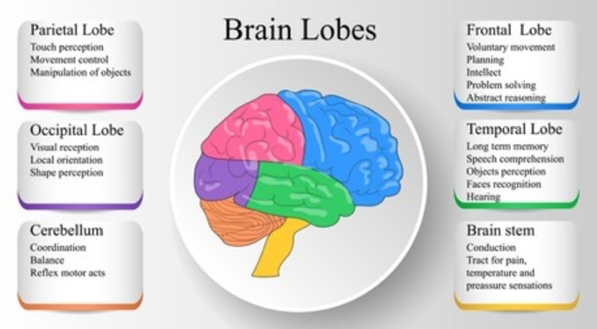
The stage at which the brain damage that causes cerebral palsy occurs, will determine the brain’s development at time of injury and therefore the symptoms and type of Cerebral Palsy (CP). Most cases of CP can be traced back to common maternal health problems during pregnancy, but whatever the cause may be, there will be some impaired function, ranging from relatively unnoticeable minor issues to mental and physical debilitation, depending on the area and extent of brain damage.
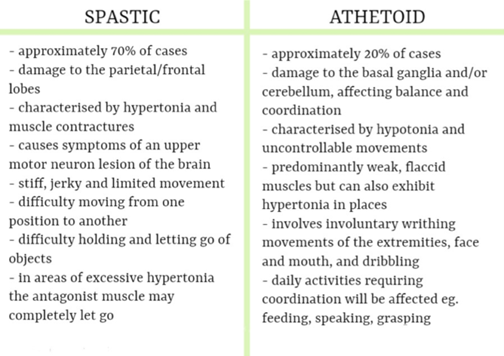
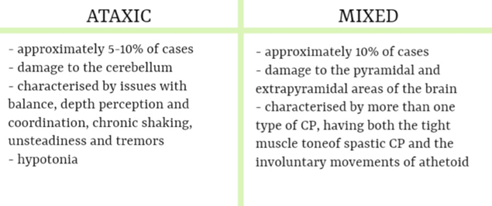
The area of brain damage will determine how the CP affects movement, posture and muscle coordination, and the range of symptoms and their severity is extensive. In addition to the type of CP cases will be classified by the area of the body that is affected
• hemiplegic – the left or right side is affected
• diplegic – either two arms or two legs are affected
• quadriplegic – all the extremities are affected to some extent
CP is not a progressive disorder, although the type may change with age, so if symptoms worsen significantly, other CNS dysfunctions should be explored
Symptoms usually become noticeable from around 6 months old, when voluntary motor skills start to develop. Adults with CP tend to age faster due to muscle fatigue. Treatment is focused on managing symptoms to improve functionality, for example, speech therapy, occupational therapy, physiotherapy etc
Most children with CP have at least one health issue caused by or connected with cerebral palsy, and approximately 35% of children with CP will experience seizures of some kind.
Treatment of CP is about managing symptoms to enable maximum functioning and quality of life, for example, with my daughter who had spastic diplegia, the main goals were improving her gait patterns by working on reducing muscle contractures, and working on her bowel to prevent obstructions, although there were, of course, many other treatment goals.
In this list of the most common treatments and therapies for CP, you will notice that massage therapy is not included. Unfortunately it is something that is overlooked, yet could provide valuable and accessible therapy in many CP cases. One of the difficulties that I, and many other parents of children with CP face, is the struggle to be able to either afford or access local treatment to supplement the limited resources of the NHS. Accessing therapy for my daughter above the standard therapies and what I carried out at home every day, would often involve having to apply for grants to be able to pay the hundreds of pounds that treatment cost or driving up to four hours for appointments.
This is physically, emotionally, mentally and financially draining. Yet I started to massage my daughter regularly, both to help ease the contractures and spasticity, and also to prevent bowel obstructions, when the milder laxatives started to be ineffective and thus the need for suppositories was becoming more necessary.
Let’s face it, nobody likes to use suppositories, they can cause severe stomach cramps and are just not pleasant. I was seeing that by giving her abdominal massages roughly every couple of days, she was not suffering from constipation because the peristaltic movement of her bowel was stimulated, and she did not require the suppositories that she hated so much. Also, by working daily on her legs the spasticity reduced, improving her gait patterns and eventually she surpassed medical expectation and began to walk independently around our home.

However, in order to be able to offer this to clients with CP, it is essential that further training is undertaken and time spent around people with CP to really understand the gait patterns, i.e. spastic hemiplegia and spastic diplegia.
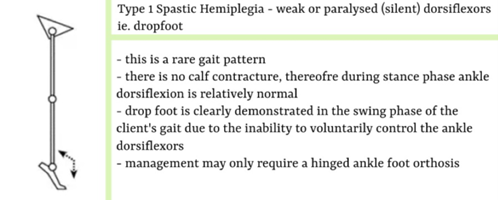
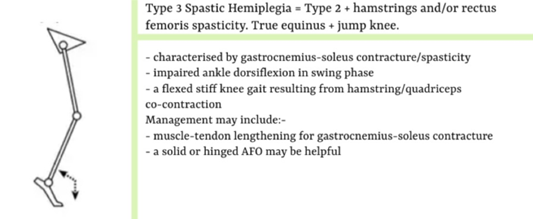
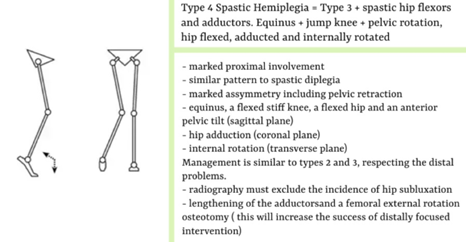
Spastic hemiplegia can be classified as four types each with a different pattern in the sagittal plane. Limb length discrepancy is a common characteristic of types 2, 3 and 4 with the hemiplegic leg being shorter.
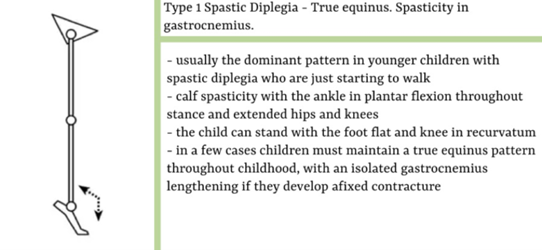
Type 2 hemiplegia is the most common type.Type 2 =type 1+ triceps surae contracture.
True equinus is noted in the stance phase of gait because of the spasticity and/or contracture of the gastroc-soleus muscles. There are two sub-categories to type 2 hemiplegic gait patterns, which are:
- Equinus plus neutral knee and extended hip.
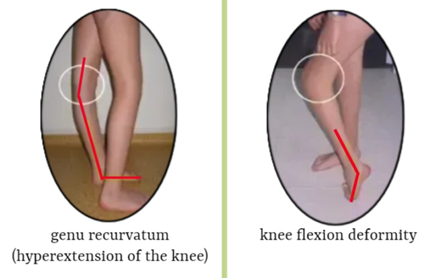
- Equinus plus recurvatum knee and extended hip
There is usually a variable degree of drop foot in swing because of impaired function in tibialis anterior and the ankle dorsiflexor. A pattern of true equinus can be seen, with the ankle in the plantar flexion range through most of the stance phase. The plantar flexion / knee extension couple is overactivee and the knee may adopt a position of extension or recurvatum.
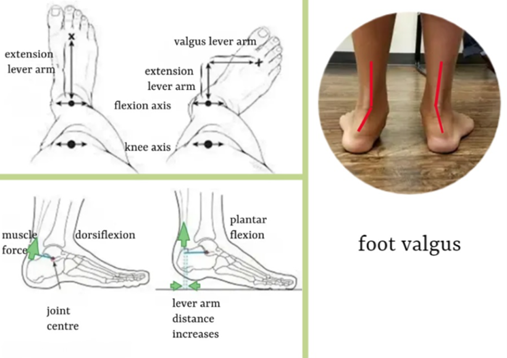
Spastic diplegia often involves three types of deformities, collectively known as lever arm
disease. Management will often involve rotational osteotomies and foot stabilization surgery.
- musculo-tendinous contractures
- torsional deformities of the long bones
- medial femoral torsion
- lateral tibial torsion – presents as out-toed stance and gait pattern
- foot deformities
- midfoot breaching – presents as out-toed stance and gait pattern
- foot valgus and abduction

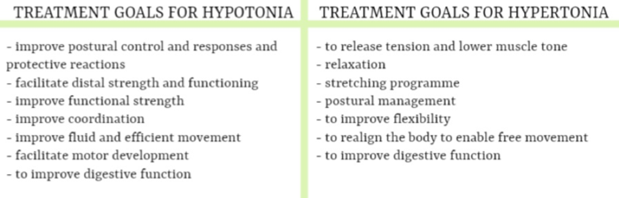
In addition to understanding the various gait patterns, a therapist must also know the difference between hypotonia and hypertonia, and what that means in terms of adjusting a treatment.
Muscle tone is the potential ability of a muscle to counterbalance an outside force or stretch. through balance responses, righting reactions (responses of the head and eyes to the body processing sensory input from the visual and vestibular systems) or protective reactions, and to relax as soon as the perceived change is gone.
With CP (particularly athetoid) related hypotonia the muscles are slow to contract against an outside force and unable to sustain a prolonged muscle contraction, due to disruption in the nerve pathways of the central nervous system, which transmit messages from the brain to the body to activate/deactivate muscle activity. This results in weak, flaccid muscles, or poor muscle tone and posture. Massage can reawaken a muscle by flooding it with sensory information, developing the brain’s recognition of changes in muscle length and helping to transmit messages to the brain to initiate a muscle contraction. Regular treatment brings the potential to elicit more regular responses and improve hypotonic muscle function, improving fine motor control and overall body strength.
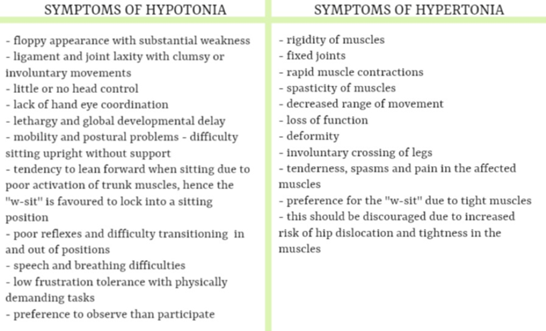
With hypertonia that generally occurs in spastic CP, the brain damage overstimulates the nerves or interrupts the signals to the muscles to contract, resulting in stiff arms and legs. Massage can help to reduce tension within the muscles and improve their ability to stretch, thus helping to prevent contractures, which lead to reduced range of movement and loss of function.
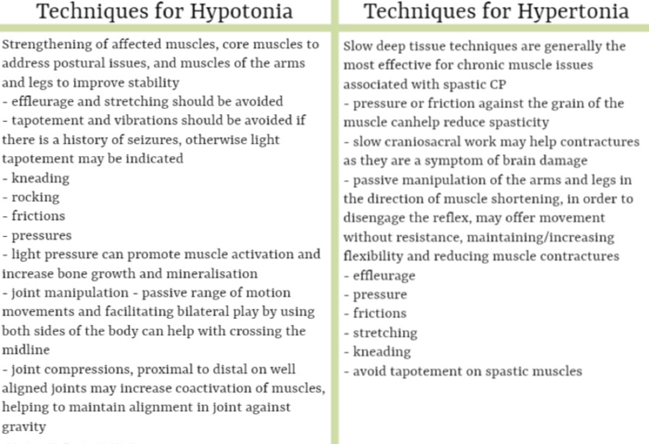
The techniques used in massage for the client with cerebral palsy will depend on the type of CP and whether the muscle tone is high or low. Treatment will be a slow process so perseverance is key, but by sustaining the same activity, but modifying where necessary, muscle activation and fluid movement can be achieved to various degrees.
Massage can undoubtedly reinforce physiotherapy and other services and be very successful in improving the quality of life of a client with CP, but some adjustments in the delivery of treatment may be required. As therapists we have many methods at our disposal to achieve results, but slow deep tissue techniques are generally the most beneficial for chronic muscle issues related to CP. Application of pressure or friction against the grain of the muscle can effectively reduce spasticity in children with cerebral palsy. However, we must remember that the muscle and connective tissues are not the root of the problem. Contractures are a symptom of the damage in the brain, so stretching the muscles and fascia alone will simply bring about either no progress or a very short lived improvement. Therefore slow craniosacral work and passive manipulation of the arms and legs in the direction of muscle shortening, in order to disengage the reflex, will offer the client improved movement without resistance. Initially treatment will be somewhat experimental to find out what techniques are relaxing for each client.
Application of different methods will be required to achieve positive outcomes for CP patients, who will exhibit a whole array of symptoms. However, care must be taken when using mechanical aids as, while they may help to reinforce results, they tend to enable a much higher level of pressure without much effort and this could over stimulate the muscle.
There are, as with any massage, contraindications that should be noted, and liaising with the child’s paediatrician and therapy team before starting any massage treatments is essential, because in some circumstances it would not be advised.
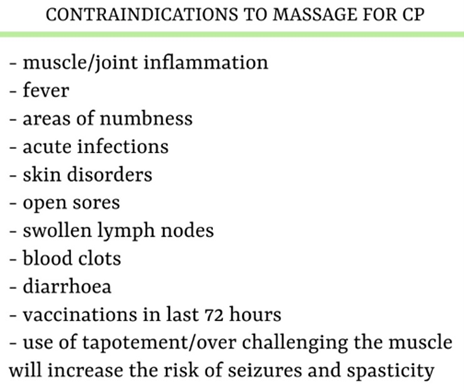
When treating a client with CP, therapists really just need to give extra consideration to the usual precautions that they would with any other client, such as not overworking the muscles or working on numb areas. If the symptoms worsen, you must take a different approach.
Particular considerations are
Being aware of any medical aids such as feeding tubes and avoiding massage directly in that are
Having extra awareness of the room temperature. This is important to promote relaxation, particularly in those with spastic CP who tend to have a very high metabolism, and use energy at a much faster rate, making them prone to feeling cold
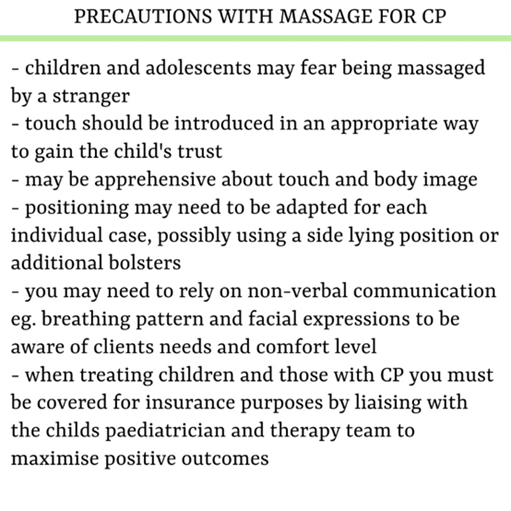
Being sensitive to the fact that children with CP are often subjected to numerous painful and intrusive medical procedures where they are handling rather than touch, causing fear of being touched by a stranger.
Benefits to Quality of Life
 Massage therapy can make a huge difference in the quality of life of a child with CP, reducing physical symptoms, improving cognition and social interaction, and we, as therapists are in a privileged position to be able to offer a treatment that isn’t painful or intrusive, and can bring about a good night’s sleep, improved breathing or better posture.
Massage therapy can make a huge difference in the quality of life of a child with CP, reducing physical symptoms, improving cognition and social interaction, and we, as therapists are in a privileged position to be able to offer a treatment that isn’t painful or intrusive, and can bring about a good night’s sleep, improved breathing or better posture.
In addition to generally improved wellbeing, there are numerous physical and psychosocial benefits of massage for those with CP.
However, passive stretching alone is not effective for long-term improvement in muscle tightness for children with cerebral palsy, but paediatric Instrument assisted soft tissue mobilisation (IASTM) can further reduce spasticity and contractures by improving mobilisation of restricted tissue and increasing range of motion and flexibility. This method has been shown to be particularly successful in improving “locked” hips and pelvis, inward turned ankles, crossed knees and thighs while walking and feet planting on the ball of the foot rather than the heel, all of which are signs of tight adductors.

In taking the decision to treat clients with cerebral palsy, it is vital that the therapist understands that learning extends beyond the training course. There is nothing quite like working with disability to bring out judgements that we didn’t even realise were within us, and society naturally fears what they don’t understand or people that look different. It can be daunting to communicate with someone who can’t speak and has a drooling problem. We can develop our knowledge through training, but it’s really not until we go into practice and start treating people that all of that knowledge starts to make sense, so we should embrace these challenging learning opportunities. Much of what you will learn about CP will come from each client’s view of themselves and their condition.
My advice is that if you are wanting to move into treating clients with CP, before taking on any clients, you should not only undertake a training course, but also volunteer at some groups such as Whizzkidz wheelchair skills days, Wheelpower sports camps for disabled children or even with physiotherapists at the local children’s centre.
