Little Leaguer's Elbow

LITTLE LEAGUER’S ELBOW/ MEDIAL EPICONDYLE APOPHYSITIS
Research has shown that at least 25% of baseball players aged 9-12 years old suffer with elbow pain, or Little leaguer’s elbow, which is an overuse injury that causes pain on the inner elbow. The umbrella term “Little league elbow” incorporates:-
- delayed or accelerated growth of the medial epicondyle
- medial epicondlyar fragmentation
- medial epicondylitis
The growth plates are still maturing during adolescence, and are therefore weak and prone to injury. While medial epicondyle apophysitis (chronic inflammation of the growth plate), is the most common injury, there may also be lateral or posterior injury. Presentation is usually dependant on age with younger children (under 10 years old) suffering with medial epicondyle apophysitis, and older children being more prone to epicondylar avulsion fractures.
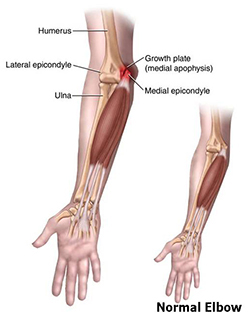
The elbow joint is comprised of three bones – the humerus (upper arm) and the radius and ulna (lower arm). The ulna forms the medial elbow and creates the tip (olecranon) of the elbow. Forearm muscles attach to the medial epicondyle helping to stabilize the elbow when throwing, alongside ligaments.
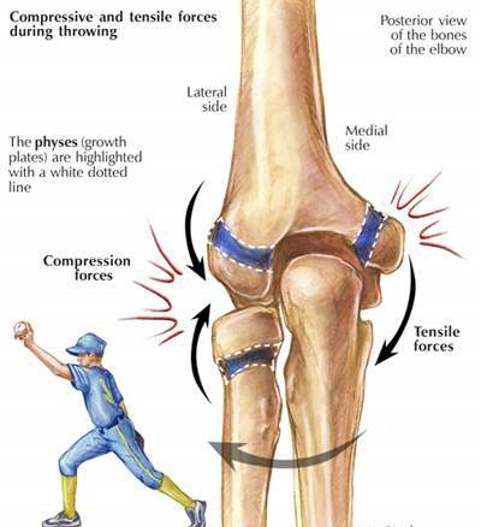
Increased tensile forces on the medial growth plates during the late cocking and early acceleration phases of a throw result in high compressive forces on the lateral elbow. Injury occurs when these forces repeatedly cause microtrauma, or due to poor technique.
(The cocking phase: the front foot makes contact with the ground and the pitching arm abducts and extends as far as possible behind the body. The shoulder is in maximum external rotation, the elbow is flexed, and the forearm is supinated, meaning that the deltoid, rotator cuff, and elbow musculature are very active. The acceleration phase: the throwing arm starts to internally rotate and adduct, while the elbow extends, concluding with the release of the ball. A large valgus force stresses the medial ligaments at the elbow. )
RISK FACTORS
- pitchers aged 9-14 years old have the highest risk of medial epicondyle apophysitis
- any athletes who throw overhead
- overuse injuries affect:-
- 2-8% of baseball players overall
- 20-40 % of children aged 9-12 years old
- 30-50% of adolescents
- an adolescent baseball pitcher who throws too many pitches too frequently, exceeding the force that the growth plate is able to withstand
- certain pitches eg. curveball, breaking pitches increase stress on the immature elbow
CAUSES
- repeated overhead throwing with improper mechanics, or lack of muscle strength and endurance
- high valgus torque of the throwing motion and tensile stress at the elbow
- repetitive trauma to the hypertrophic zone of the apophyseal cartilage
- throwing breaking pitches and curveballs too young
- increased pitching counts
SYMPTOMS
- medial elbow pain
- inflammation
- reduced throwing speed or distance
- point tenderness
- effusion ie. fluid moving into the soft tissues
- flexion contracture (noted up to 15 degrees)
- widening and/or fragmentation of apophysis
- possibly compression growth plate injuries on lateral side
- possibly posterior medial impingement
- in severe cases avulsion fractures

TREATMENT
Early treatment can improve outcomes and reduce the risk of permanent damage or functional disability. While research has shown that medial epicondylar fractures of more than 5mm will generally require surgery, there has also been an argument that conservative management has similar long-term results.
- Avoid throwing for 4-6 weeks to allow the growth plate heal
- Ice packs can be used to reduce inflammation
- Anti-inflammatories
- physical therapy to work on muscle strength and endurance, and therefore reduce the stress on the growth plate and re-injury
- work on core and hip/trunk stability to avoid compensatory stress by the elbow
- elbow extension brace if a flexion contracture is presentimmobilization in severe cases
SURGICAL TREATMENT
Surgery in adolescents is advised if there are:-
- Loose cartilaginous bodies which catch or impede elbow motion
- Avulsion fractures
- Osteochondritis dissecans - bone underneath the cartilage dies due to reduced blood flow, resulting in bone and cartilage breaking away, causing pain and restricting movement
- As a last resort when conservative treatment has not improved symptoms
RECOVERY FROM MEDIAL EPICONDYLE APOPHYSITIS
- stop any activity that increases stress on the medial elbow
- in early stages where pain is minimal, reduce level, duration, and frequency of throwing
- in severe cases immobilization may be advised
4-6 WEEKS
- wrist and elbow extension and flexion, forearm supination and pronation when pain levels allow
- elbow and wrist flexion and extension eccentric exercises: high repetitions with low load to improve localized circulation during tissue healing
- resisted elbow flexion and extension, with theraband or cuff weights
When the above exercises can be done pain free, progress to throwing-specific exercises.
12 WEEKS
- avoid high stress pitches
- stay within an appropriate number of pitches
- maintain a core and shoulder strengthening program throughout the year to maintain/improve strength and muscle control
MASSAGE THERAPY
Working on the rotator cuff muscles which stabilise the shoulder will be beneficial. Trigger point therapy applied to the wrist flexors has been found to be particularly effective in terms of pain relief and accelerating the healing process.