- 07736 104738
- sam@medicalmassagelady.com
- Mon - Sat, 8:00 - 18:30

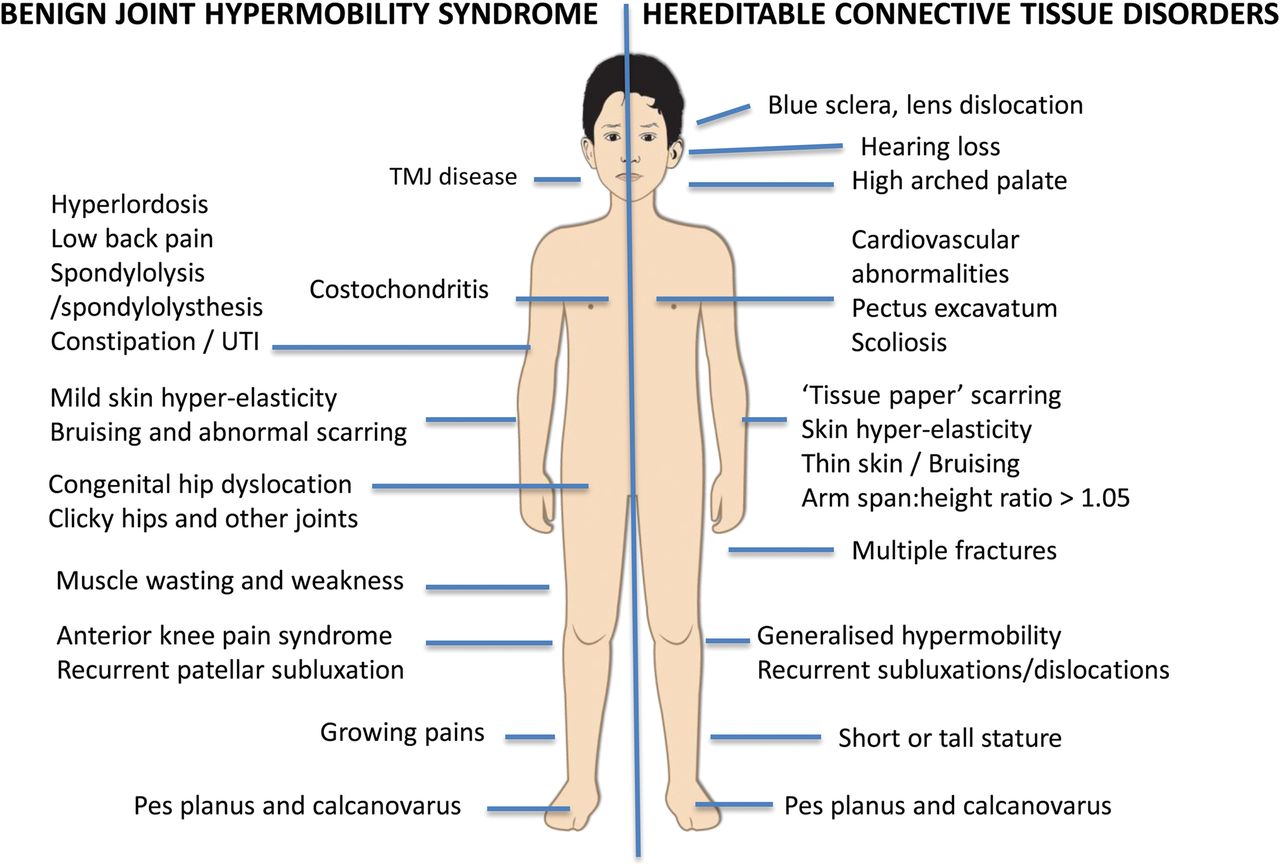
Hypermobile Ehlers-Danlos syndrome is one of the most common disorders of the connective tissue, and while it doesn’t impact on life expectancy, it can greatly impact on quality of life and everyday functioning as a result of musculoskeletal pain and joint instability. In the absence of specific diagnostic tests, indicators of hEDS will include :-
• joint hypermobility
• musculoskeletal problems such as chronic pain and dislocations
• family history
• signs of faulty connective tissue throughout the body With numerous complications of hypermobility and even the presence of hEDS related musculoskeletal issues still not confirming a hEDS diagnosis, reference to a hypermobility spectrum is becoming more common.
CAUSES:-
The underlying cause of hEDS is usually not known, but the following causes have been suggested:-
• genetic predisposition through family member
• new mutation of the TNXB gene, inhibiting tenascin-X protein and affecting elastin fibres
• defective collagen protein
SYMPTOMS:-
• joint hypermobility
• chronic musculoskeletal pain
• dislocations/subluxations (particularly in shoulder, knee and lower jaw)
• curvature of the spine
• poor sense of body position
• degenerative bone disease/early onset arthritis/osteoporosis
• prone to injury
• slightly elastic, smooth skin
• easily bruised
• fatigue
• acrocyanosis – mottled blue colour to hand,feet and face
ASSOCIATED SYMPTOMS:-
These symptoms are not a direct result of joint hypermobility and are not a diagnostic factor, but have been linked to it:-
• Cardiovascular issues eg. mitral valve prolapse, aortic root dilatation, orthostatic tachycardia (feeling faint upon standing from lying down)
• digestive disorders, dysmotility, bloating, nausea, vomiting, heartburn, constipation, hiatus hernia
• pelvic and bladder dysfunction, pelvic prolapse, dysmenorrhea, painful intercourse
• high risk of complications in pregnancy eg. premature rupture of membranes, rapid labour and delivery (less than 4 hours)
• anxiety disorders and depression
• sleeping problems
• dysfunction of the autonomic nervous system
DIAGNOSIS:-
As stated, there is no specific test to diagnose hEDS so it usually depends on 3 criteria:-
1)generalized joint hypermobility will be assessed using the Beighton Score system
2) 2 or more of the following groups must be present :-
A)at least 5 of the following systemic manifestations of a more generalized connective tissue disorder should be present:-
• unusually soft, smooth skin
• mild skin hyperextensibility
• atrophic scarring involving at least two sites (without the papyraceous (paper thin)scars seen in classical EDS)
• bilateral piezogenic (skin coloured) papules of the heel (where fat herniates through the dermis)
• unexplained striae rubrae (stretch marks) at the back, groins, thighs, breasts and/or abdomen
• dental crowding and high or narrow palate • recurrent abdominal hernias
• pelvic floor/ rectal/ uterine prolapse in children, men or nulliparous women • arachnodactyly - abnormally long and slender fingers, in comparison to the palm of the hand and arch of the foot
• arm span-to-height ratio ≥1.05
• mitral valve prolapse
• aortic root dilatation
B) positive family history ( ie. More than one first-degree relative diagnosed with hEDS C) at least one of the following musculoskeletal complications :-
• daily musculoskeletal pain in 2 or more limbs, for at least 3 months
• chronic, widespread pain for more than 3 months
• recurring joint dislocations/ joint instability at 2 or more sites
3)all of the following:-
• absence of unusual skin fragility
• no other inherited/acquired connective tissue disorders
• no autoimmune rheumatologic conditions
• no alternative diagnoses that would explain joint hypermobility as a result of poor muscle tone/connective tissue laxity.
TREATMENT:-
Treatment will vary according to the symptoms, but should focus on relieving the symptoms, improving functional capacity, spatial awareness and joint stability, and preventing complications, to achieve independence with a minimum of external support. Treatment options may involve:-
• pain medication
• physiotherapy to strengthen the muscles and help stabilise joints
• braces, wheelchairs and other devices to assist with joint stability
• massage therapy may help
• monitoring for aortic root dilatation and osteopenia
Treatment will aim to:-
• treat acute soft tissue lesions and injuries
• relieve pain with soft tissue work and gentle mobilisation, to support joints and tissues
• improve balance and coordination
• improve the endurance and strength of the core and joint-stabilising muscles
• educate individuals to manage daily activities and normal functioning with minimal medication
• promote an active lifestyle
• improve stamina and general fitness
• re-educate posture/gait to avoid/correct abnormalities
• coordinate with professionals e.g. occupational health, physiotherapists, school teachers, school nurses, occupational therapists etc.
PAIN MANAGEMENT:-
Rehabilitation is the best treatment due to pain resulting from musculoskeletal issues as opposed to a pathology. As muscles strengthen and joint stabilise, the pain will ease but this can be a slow process.
• Hot/cold packs on joints
• TENS machines
• Massage/trigger point therapy/myofascial release
• Relaxation techniques (to manage sleeping difficulties)
• Pacing during physical activity (to avoid disruptive flare ups)
POSTURE/MOTOR CONTROL:-
Core stability should be the primary focus in order to achieve peripheral joint control.
• individual posture re-education programme
• Motor-skill training
-exercises should focus on a specific movement to improve skill and precision
-specific, isolated, low level, skilled stabilisation training can improve activation of postural muscles more than non-isolated functional exercise. This helps to adapt brain pathways in functional activities
-should be pain-free as pain stimulates the motor cortex, encouraging protective strategies
-quality over quantity to avoid fatigue and pain which will limit performance
-should be goal-orientated
MUSCLE STRENGTHENING:-
Recurring injury or postural issues leads to chronic pain, which leads to reduced activity, which leads to muscle weakness. This is particularly common in the knees of those with hEDS where there tends to be some imbalance with the glutes.
Following this pattern of exercises can improve joint stability, muscle control and strength and help reduce risk of injury in cases of ligament insufficiency:-
• static exercises (while there is pain)
• dynamic exercises
• resistance exercises
• weightbearing exercises, for which hydrotherapy can be used if pain is an issue
EXTERNAL SUPPORT:-
Using aids and supports can cause dependency which leads to muscle weakness, but in acute stages of injury a brace support an unstable joint to improve movement and posture and consequently assist with proprioception and healing. They can also make participation in sports or other activities possible.
GAIT REHABILITATION:-
Gait will be affected by hypermobile joints and the resulting issues with proprioception, motor control, muscle weakness and reduced stamina, and this in turn changes the way someone functions, causing overloading, pain and fatigue. Gait analysis can bring recognition of abnormalities in order to improve posture. Flat feet are common in hypermobility and can change the gait, but supportive footwear/insoles can reduce the impact through the foot, reducing pain.
BALANCE AND PROPRIOCEPTION
Sensory input during rehabilitation to combat the effects of the skin laxity can be achieved by:-
• ‘hands on’ movement facilitation by therapists
• wearing tight fitting clothing
• using tape during functional rehabilitation sessions
Balance, proprioception, posture, pain and muscle strength can be improved through:-
• closed chain/weightbearing exercise
• exercises with balance board eg.squats, bridging, four point kneeling, standing on one leg
• dynamic balance activities using a Swiss ball
PSYCHOLOGICAL SUPPORT:-
• if quality of life is seriously affected by pain and functional limitations
• pain levels can be determined by the way we think so by altering pain perception through coping strategies, stress and sleeping patterns can be improved
EXERCISE FOR hEDS
While exercise is the best treatment for hEDS, each person will have different symptoms with different levels of functioning, and so it is important to choose the right kind of exercise in order to avoid pain and injury. Many will lead a more sedentary lifestyle due to muscle weakness and pain, but this will simply worsen the condition of the muscles and reduce functioning further. If there is muscle weakness one must be cautious and begin with low impact exercise as moving too quickly may encourage flare ups. The idea is to find the balance between maintaining lifelong fitness through healthy physical activity to reduce pain, and improve muscle strength and joint stability, and high impact physical pursuits which can result in a chronic pain cycle and disability.
DO:-
• swimming, aqua aerobics or running in deep water will improve cardiovascular fitness without too much impact on the joints and offers a full body workout
• Tai Chi and pilates will improve balance and core stability
• cycling offers aerobic exercise without too much stress on the joints
• elliptical training allows cardiovascular exercise without high impact on the joints - treadmills, steppers and stationary bikes
• nordic pole walking is functional, improves proprioception and core stability
• free weights strengthen deep stabilizer muscles which are particularly important in hEDS, and which are often forgotten. Unlike machines, they allows the body to work on more than one axis, however, it is easier to make mistakes, so is important to progress slowly.
MAYBE:-
• Yoga – while joint hypermobility means that you are flexible, yoga can put you at higher risk of joint subluxation. It can be done and improve balance, but best to find an instructor who has knowledge of hypermobility.
• Non-contact team sports: The jury is still out on soccer, tennis, volleyball, and the like. The effect of this type of sport varies from one person to the next, depending on how EDS affects your body. The best advice I can give you here (which more or less applies to everything on this list) is this: don’t make your decision based on the opinion of one rare disease writer on the internet– talk to your doctor, your physical therapist or specialist if you have one. Reflect back on your own life, your injuries and recovery. EDS manifests differently in every patient, and your experience might be totally different than someone else’s.
DON’T:-
• Contact sports eg. football, hockey, rugby, aggressive trampolining and anything that involves tackling due to increased risk of injury and difficulties healing
• Competitive gymnastics or cheerleading are best avoided if unsure whether flexibility is due to stretching your muscles or stretching your already lax tendons and ligaments
• Stop because of mild to moderate pain as exercising with EDS may hurt, so it’s good to push through some pain to strengthen the muscles and reduce chronic pain. However, you should know your limits and if something really feels wrong it’s time to stop
• Distance running – using an elliptical treadmill will place less stress on your joints
• Olympic lifting and cross-fit – high intensity workouts will simply increase the risk of a flare up and push you into a chronic pain cycle
BENEFITS OF MASSAGE FOR hEDS
• relieve muscular tension and pain
• improve ability to distinguish between different sensations
• improve sensitivity around scar sites by reducing adhesions
• muscle fatigue often associated with physical exertion
• reduce muscle spasms caused by overuse from compensating for weakened ligaments and tendons
• general relaxation
• relieve discomfort from skin hypersensitivity
• improve proprioceptive awareness of the body by helping to retrain the nervous system
CAUTIONS:-
• ensure you see a fully qualified and registered therapist
• limit the first appointment to one specific area for which you can assess the effects of the treatment
• massage should not be deep
• ensure that your therapist listens to your feedback It is important to do strengthening exercises following massage and joint realignment or the joint will be vulnerable and the muscle spasms will start again.


